
 Book a Demo to Build Your Team Today!
Book a Demo to Build Your Team Today!
On-Demand Outsourcing BPO Services for Healthcare Providers With 24/7 Coverage!
Save up to 70% on staffing costs!
Browse Specialty Staffing ServicesSummarize this blog post with:
PHARMACIST CLINICAL REVIEW PROCESS

Author: JYOTHIKA TUNGUTOORI
ABSTRACT
Background:
Clinical pharmacy services have potential to contribute significantly to the multidisciplinary acts providing safe and effective economic care for patient. The aim of this review is to appraise, and present the available evidence of the characteristics and outcomes of clinical pharmacy practice as part of a multidisciplinary care of patients with treatment regimens for infectious, uncurable and life-threatening diseases like advanced cancer and chronic kidney disease and to ascertain their feasibility and acceptability.
The clinical role of pharmacist is expanding as in the use of clinical guidelines as they perform review of drug therapy which helps to recognize and utilise relevant clinical and lab data to identify and resolve drug related problems. The objectives are to describe the implementation strategies used, describe the resulting outcomes and to access the effectiveness of strategies. This describes the concept of clinical medication review by the pharmacist based on diseased patients directing towards their treatment. The clinical and medication review and supply by the pharmacist involves both cognitive and the technical skills related to the safety and appropriateness of prescribed medicines. The insight of this study have implications for enhancing awareness of decision making process in pharmacy practice and assessment approach in medication supply.
Purpose: The implementation, and challenges of clinical pharmacist services within a precision medicine programme for cancer patients and CKD patients.
Introduction: The clinical pharmacist play a significant role in treatment regimen of patients ongoing difficulties. Cancer patients are vulnerable to drug interactions, which may alter the efficacy and toxicity of treatment, leading to severe clinical consequences. Over half of the patients are experiencing the poor controlled pain during their last year of life. Besides clinical pharmacist, community pharmacist are most frequently seen with cancer patients. Patients perspectives are often difficult to obtain post interventions from patients with advanced disease due to rapid deterioration. This shows that pharmacist educational interventions are potentially beneficial for patients with cancer pain.
Chronic Kidney Disease (CKD) continues to be a global concern with a high risk of mortality, and reduced life expectancy. Clinical pharmacy has the potential to contribute significantly to the multidisciplinary team providing safe, effective and economic care, as the key roles of these are included in specific areas as in renal mineral bone disease, another major role is to contribute to renal drug cost management. The specific aim is to know the activities performed (processes, medication review, prescribing) and when they are performed. Hence, the evidence of pharmacist interventions in patients with CKD is scarce, of variable quality and heterogenous outcomes.
Methodology:
Treatment regimen for cancer patients by clinical pharmacist:
- 1. Study designs and settings: This is a retrospective study regarding the clinical assistance of pharmacist to patients with thoracic cancer who received cancer chemotherapy. One of the two clinical pharmacist in charge, including oncology pharmacist specialist and implemented pharmaceutical care for the patients. Adverse events where monitored in cooperation with clinical pharmacist and physicians.
- Cancer chemotherapy: All thoracic cancer chemotherapy is administered based on a treatment protocol agreed upon by the clinical pharmacist in advance. Standard antiemetic medication is administered based on the clinical oncology guidelines. patients who got developed with chemotherapy-induced nausea and vomiting were prophylactically administered, olanzapine, lorazepam in addition to standard prophylactic antiemetic therapy.
Standard chemotherapy order forms containing the dosage of anticancer drugs and dose calculation(mg/m), start date and time, day of therapy, infusion rate and duration of infusion, route (intravenous infusion), frequency of anticancer administration, and prophylactic support care restricted to injections entered for each regimen.
Challenges and duties of clinical pharmacist:
Pharmacist interview all patients on admission and check over their verified prescription to assist their treatment regimen. Patients’ medication history is stored, daily review of laboratory data, provided drug information to medical staff and patients education is recorded.
The monitoring and reporting adverse reactions, patient counselling, drug interactions, appropriate dosages, dose intervals and route of administration is patiently determined. All these interventions performed by pharmacist will be recorded and guided to patients.
Results:
Toxicities of targeted therapies: The idea that targeted therapies ate toxic has strong consensus that arose among clinical pharmacist.
High cost and equality of access: The high cost of targeted therapies, or equity of access, is a theme raised. pharmacist expressed concern about public funding for potentially effective drugs in patient groups. The cost factor imposed greater scrutiny of the risks and benefits of individual being treated with particular agents.
Role for all pharmacist? Pharmacist saw targeted therapies as something with which most pharmacist would never deal or something that required handling by only appropriately trained pharmacists, initially and the clinical pharmacist indicated that handling targeted therapies is a role for all pharmacists.
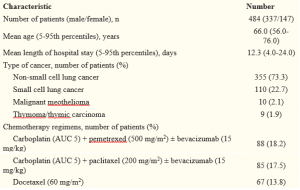
Patient demographics: The hospitalised patients for the purpose of cancer chemotherapy are enrolled here as mentioned below.
Patient demographics –
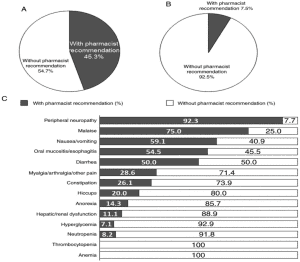
Drug specific interventions by clinical pharmacist before administration of chemotherapy:
The various types of interventions implemented by the clinical pharmacist before the administration of chemotherapy is mentioned below as –
The most frequent type of intervention was drug addition among all the various interventions followed.
| Category of intervention (n) | Contents of intervention (n) |
| Drug addition (82) | Antiemetic drugs (26), vitamin B12 or folic acid on pemetrexed chemotherapy (18), zoledronic acid or precipitated calcium carbonate/cholecalciferol/magnesium carbonate for high blood calcium due to cancer (14), hydration on cisplatin chemotherapy or renal dysfunction (12). |
| Drug dose adjustment (27) | Anticancer drugs (22), other drugs (5) |
| Drug selection (15) | Antiemetic drugs (7), anticancer drugs (8) |
| Drug discontinuation (12) | Antiemetic drugs (7), anticancer drug (2), other drugs (3) |
| Examination addition (6) | Urinary protein examination on bevacizumab chemotherapy (3), others (3) |
| Drug selection | Antiemetic drugs, anticancer drugs |
| Drug dose adjustment | Anticancer drugs, other drugs. |
-Incidence and influence of adverse events:
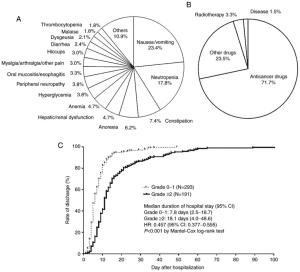
A: Types of adverse events B: causes of adverse events C: Duration of hospital stay
Interventions of adverse events:
2. Clinical pharmacist care in chronic kidney disease patients:
The case study of patient is performed and reported as- The 60 years old patient got admitted into a multidisciplinary hospital with the chief compliments of Confusion, fever, for 3 days she has medical reports and the clinical, laboratory findings of patient is found to be as below-Temp-100F, BP-190/40mmHg, pulse-85/min, WBC – 15000cu/mm.
Clinical symptoms:

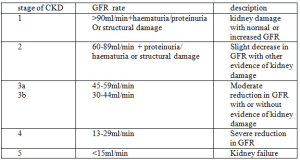
Classification of chronic kidney failure:
Clinical pharmacist treatment and counseling regimen to the patient:
Diet: A healthy diet is important is important for preventing chronic kidney disease. It lowers the amount of cholesterol in blood and keep blood pressure at healthy level. The balanced diet also includes the fresh fruits and vegetables and whole grains by avoiding food that has high levels of saturated fat as that increases the level of cholesterol.
Alcohol: Consuming the excessive amount of alcohol will cause a rise in bp, as well as raising cholesterol levels in blood. Therefore, sticking to the recommended alcohol consumption limits is best way to reduce risk of developing high bp(hypertension) and CDK.
Exercise: Regular exercise will help lower blood pressure and reduce risk of developing CKD. At least 150 minutes (2 hours and 30 minutes) of moderate-intensity aerobic activity (i.e., cycling or fast walking) every week, is recommended as per the assistance of the clinical pharmacist. Avoid nephrotoxins example: NSAIDS etc.
Food that can be prescribed and assisted to be taken by CKD patients involve the lower cholesterol and high in unsaturated fat included as – avocados, oily fish, rapeseed oil, olive oil, nuts and seeds.
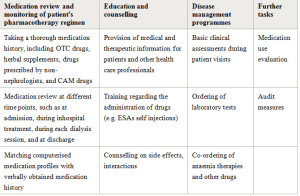
Comprehensive listing of clinical pharmacist activities performed in CKD:
Interactions and survey details:


This is the survey conducted from my college to enhance the effectiveness of pharmacist regarding the above-mentioned chronic effective diseases.
Limitations: There are several limitations here as related to the described content as the patient population is limited to inpatients with thoracic cancer receiving cancer chemotherapy
Discussions: The clinical pharmacist interventions for the prevention and treatment of adverse events in hospitalized patients with thoracic cancer receiving cancer chemotherapy. The interventions were implemented by single clinical pharmacist before the administration of cancer chemotherapy. As the targeted cancer therapies are typically expensive, this has set the criteria for starting treatment, dose reduction, drug withdrawal and prophylactic care. As a result all patients received the appropriate dosage of anticancer drug and prophylactic supportive therapy . Therefore, prevention or relief of adverse events may lead to reduced hospitalization periods.
It is therefore evident that this is been a limited amount of high quality for the benefits of clinical pharmacy practise in CKD. Despite this criticism there is a growing body of information in relation in some aspects of clinical pharmacy practice that offers some insights to the developing quality and significant differences to the outcomes of patients.
Implementing role of clinical pharmacist in trending era:
Pharmacist plays , emerging role in upgrading services and enrooting patients to their treatment regimens as, pharmacist lead a vital role in most critical days of survival. Patients with cancer these days undergo chemotherapy for their survival besides all the side effects. As of todays upgrading educational economy there is chance of implementing various different ways of rendering the disease like oral administration of drugs besides chemotherapy to escape from all the side and adverse effects which can easily available at affordable prices and ease of intake is found.
CKD these days has become a trending disorder. It has become difficult to undergo the process of dialysis to old-age people as their level of immunity and resistance decreases with ages. There is a chance to establish some kind of remedies like use of precision medications which demonstrates a higher level of effectiveness, and increased focus on R&D value. To overcome this kind of disorders, pharmacists are planning kind-of easy routes for dialysing processes and new models of care delivering.
Conclusion: The incidence of drug interactions in cancer patients is high and the pharmacist as a member of a multidisciplinary team, can contribute significantly. pharmacist are the ideal professionals to interpret results and provide counseling for patients to assist them in compliance with targeted cancer therapies and correct use of this therapies. The success of integrating this precision medicine pharmacist into a newly formed precision medicine program as this service highlights the importance of pharmacist care. Oncology clinical pharmacist seek to integrate into precision medicine programs directing care and develop knowledge where the consultations were feasible to deliver. Hence patients found this acceptable. Pharmacist medicines consultations were able to identify a substantial number of DRP’s in patients with advanced cancer care. problems with inadequate pain relief and associated side effects are most prevalent and majority of these could be addressed by pharmacist even in patients already receiving palliative care.
The pharmacist interventions improved patient’s clinical outcomes. This also shows that positive contributions of pharmacist involvement in the multidisciplinary team to provide care to patient with CKD, from the case study detailed above it is clear that, patient was given complete course and counseling for chronic kidney disease and problems get solved.
Hereby, it shows the essence of pharmacists in area of patient care and quality treatment in present scenario to expect quality of life.
References:
- Hall WD, Ward R, Brien J-E, Lu CY. Tailoring access to high-cost, genetically targeted drugs. 2005;182(12):607–608. [PubMed] [Google Scholar]
- Pharmacogenomics: a primer for policymakers, National Health Policy Forum.
- CS. Managing oral chemotherapy: the healthcare practitioner’s role– 2007;64(9:S25–S32. [PubMed] [Google Scholar]
- DL. Oral chemotherapy medications: the need for a nurse’s touch.2007;11(6):793–6. [PubMed] [Google Scholar]
- Faithfull S, P. Implementation of capecitabine (Xeloda) into a cancer centre: UK experience. 2004;854–S62. [PubMed] [Google Scholar]
- Boyle D, J. Enhancing patient adherence to improve outcomes with oral chemotherapy. Proceedings from a symposium at the 2007 /Oncology pharmacy association annual conference. 2007;32(10):1–8. [Google Scholar]
- CS. Managing oral chemotherapy: the healthcare practitioner’s role.2007;25–S32. [PubMed] [Google Scholar]
- Corner J, Halliday D, Haviland J, Douglas HR, Bath P, Clark D, et al. Exploring nursing outcomes for patients with advanced cancer following intervention by Macmillan specialist palliative cares.
- Ziegler LE, Craigs CL, West RM, Carder Martin P, et al. Is palliative care support associated with better quality end-of-life care indicators for patients with advanced cancer. A retrospective cohort.
- Brant H, Atherton H S, McKinstry B, Campbell JL, Salisbury C. Using alternatives to face-to-face consultations: a survey of prevalence and attitudes in general practice. Br J Gen.
- JC, Brown CM, Lawson KA, Godley P, et al. Patient satisfaction with a pharmacist-provided telephone medication therapy management program.
- Eldridge S. Can a self-management program delivered by a community pharmacist improve asthma control? A randomized trial. Thorax. 2003;58(10):851–4.
- White CD, Hardy JR KS, Charles MA, Pinkerton CR. Randomized controlled trials of palliative care—a survey of the views of advanced cancer patients and their relatives, Cancer.
 Read Case Studies
Read Case Studies 
Ready to Build Your Team?

Categories

Recent Posts
- Revenue Cycle Management: The Complete Guide to Maximizing Your Practice’s Financial Health
- Prior Authorization Is Costing Your Practice 16+ Hours Per Week: Here’s How to Fix It
- How AI Voice Bots Are Fixing the Healthcare Front Desk?
- How To Cut Claim Denials In Half Without Adding More Staff?
- How AI Chatbot Services Are Redefining Patient Communication for Clinics?

 Virtual Medical Assistants
Virtual Medical Assistants Insurance Verification
Insurance Verification Prior Authorization (AI)
Prior Authorization (AI) Medical Scribing (AI)
Medical Scribing (AI) Telemedicine Services
Telemedicine Services Medical Data Entry
Medical Data Entry Medical Coding
Medical Coding Revenue Cycle Management
Revenue Cycle Management




