

Author: RAMKUMAR S & MYTHILI S
ABSTRACT:
Electronic health records is a computer-based program in which the collection of data is related to clinical research, clinical registry functions, administrative functions, and in quality improvement. This is done by NPL (natural processing language) in the linguistic information is converted into a structural form or in the form of code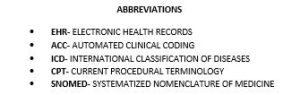 i.e numerical form this process of converting the information into a structural form is known as clinical coding this clinical coding is classified into manual coding and automated clinical coding, in Which the manual coding is human-based and automated clinical coding is based on the artificial intelligence technology this also consists of different classification of coding includes ICD’S, CPT ‘S, SNOMED’S, HCPCS. This article gives a brief outline about the ICD-10, CPT, and SNOMED systems.
i.e numerical form this process of converting the information into a structural form is known as clinical coding this clinical coding is classified into manual coding and automated clinical coding, in Which the manual coding is human-based and automated clinical coding is based on the artificial intelligence technology this also consists of different classification of coding includes ICD’S, CPT ‘S, SNOMED’S, HCPCS. This article gives a brief outline about the ICD-10, CPT, and SNOMED systems.
INTRODUCTION:
Electronic health records (EHR) have become common ground in healthcare use of the electronic health record has gained a great swift over the few years(1). EHRs have been proposed as a means for improving, the availability, completeness, and legibility of patient information recording any diseases(2). Nearly 3\4 of the physicians generate reports using EHRs with this approach in the medical field is going towards electronic documentation. EHR’s recent system has tended to adopt more active roles in the clinical field(3). EHR’s system has entailed two relevant aspects. Firstly the chemical data analysis to inform the physician on their medical decisions for the patient(4). Secondly, this exploits data regarding clinical, administrative, and health which includes demographic data and prescriptions, etc…(5) Hospitals and general healthcare providers significantly use medical coding as a tool to record the diagnoses information of a patient or to record the medical services provided by the physician to the patient(6).
CLINICAL CODING:
These medical codes are used to provide access to medical records by retrieving information regarding administrative, educational and medical research(7). These codes also facilitate the payment of health services, evaluate the patient’s use of the health care facilities, study the health care cost, predict the health care trends, and plan health care tools for future needs(8). The purpose of the coding is to provide consistent and comparable clinical information about the patients in the locality over a period of time, these data are used to improve the healthcare planning and policy of the governing authority and these data help the healthcare sector to understand the epidemiological condition of a specific area(9). Classification system like ICD- 10[ International System of Classification of Diseases 10th edition] is used in the conversion of textual data into structured data. Clinical coding is a nontrivial task of collection of the data this is used for billing purposes in the US this process includes the abstraction of the data and also summarization of the data collected. The US uses ICD 10-based coding system and the UK uses NHS [ national health services] based coding system (10-13)
Figure 1 clinical coding outline
AUTOMATED CLINICAL CODING (ACC)
Automated medical coding is a part of electronic health records, this encompasses different computer-based approaches which transform narrative records into structural records these structural records include performing standard coding without human interactions(14). This system of clinical coding may be automated by the use of AI techniques ( artificial intelligence )(15). This is performed by the use of NPL & machine learning(16). AI has been a most promising approach in the field of medical coding by providing more promising data in a compact form(17). ACC is a potential AI application that is used in managing clinical records of research laboratories and in the healthcare centers (18-20)
In this paper, we summarise the ICD-10, CPT, and SNOMED clinical coding system and their use in the various medical sector.
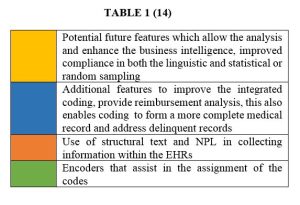
Figure 2 Automated coding workflow
ICD-10 [ International Classification Of Diseases]
ICD is a classification of diseases released by the world health organization (WHO) and this defines the universe of the disease’s injuries, disorders, and other health-related conditions and classifies the standards of the origin(21). The ICD was first published in the year 1893, ICD has become an important index in the management of medical records, administrative records, health insurance, and literature records regarding diseases(22). At present most of the institutions use ICD-10 codes which are diagnostic-related group subsidies for the inpatient who mainly rely on manual coding done by licensed & professional disease coders(23). This ICD-10 consists of more than 60,000 codes(24-27). This system is time-consuming & labor- intensive and the rules of ICD-10 are complicated even for the disease coders (21,28,29)
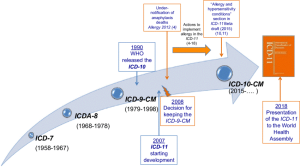
Figure 3 History in the development of ICD 10
CPT (Current procedural terminologies):
CPT was developed in 1996 by the American medical association (AMM) with data from the national medical specialty societies(30,31). This system is the most commonly used system of procedure in the billing codes for medical, surgical, and diagnostical services(31,33).CPT is also used in targeting the tissues of cancer by targeting the topoisomerase enzyme(32) and in the various diseases The CPT is classified into three categories they are
Category I CPT: these are the codes that are released annually. these codes are the distinct medical procedures which are furnished by the QHPs these codes are mostly of 5 digits.(34)
Category II CPT: these codes are the performance measurement codes. These codes are released thrice a year these are numerical alpha codes.(35)
Category III CPT: these codes are not permanent codes these codes emerge day by day due to development of new and emerging technologies to allow the collection of data and to get the assessment of the new services. These codes are released biannually. These codes are also numerical alpha codes
COMPARISON BETWEEN CATEGORY I, II & III CPT CODES
| CATEGORY I (34,36) | CATEGORY II (35,36) | CATEGORY III(36-39) |
| Describe the distinct medical procedure or services furnished by the QHP (qualified health plan ) | These are performance measurement codes | These are not permanent codes these codes emerge day by day for newly developed technology |
| These codes are released annually | These codes are released three times a year during the month of march, July and November | These codes are released biannually in January and July |
| 5-digit numerical codes | Numerical alpha codes | Numerical alpha codes |
| Only numericals (40) | 4 numerical followed by letter F (40) | 4 numerical followed by letter T (40) |
TABLE 2 CPT CODES CATEGORY I (41)
| CATEGORY I CPT CODES | NUMERICAL RANGES |
| SURGERY | 10021-69990 |
| RADIOLOGY | 70010-79999 |
| PATHOLOGY & LABORATORY | 80047-89398 |
| EVALUATION & MANAGEMENT | 99201-99499 |
| ANESTHESIA | 00100-0199; 99100-99140 |
| MEDICINE | 90281-99199;99500-99607 |
TABLE 3 CPT CATEGORY II (41)
| CATEGORY II CPT CODES | NUMERICAL CODES |
| PATIENT HISTORY | 1000F-1220F |
| PHYSICAL EXAMINATION | 2000F-2050F |
| THERAPEUTIC, PREVENTIVE OR OTHER INTERVENTIONS | 4000F-4306F |
| PATIENT SAFETY | 6005F-6045F |
| STRUCTURAL MEASURES | 7010F-7025F |
TABLE 4 CPT CATEGORY III
| CATEGORY III CPT CODES | NUMERICAL CODE |
| AUDIOLOGY CODES | 0208T -0212T(38) |
| MONO POLAR RADIO FREQUENCY | 0672T(39) |
| ULTRA SOUND GUIDED FOR FOCAL LASER | 0655T(39) |
SONMED [SYSTEMISED NOMENCLATURE OF MEDICINE ] :
The systematized nomenclature of pathology (SNOP) was first developed by the group of pathologist in the College of American Pathologists(42). This enables a consistent way of aggregating, indexing retrieving, and storing clinical data across specialties and sites of care. SNOMED also enables structuring and computerizing the medical records which reduce the variability in the way data is captured, encoded, and used for the clinical care of the patients. this also enables automated reasoning i.e in decision making(43-45). SNOMED CT is the presently used system of coding in the SNOMED classification. SNOMED CT currently consists of more than three lakh medical concepts this provides a standard by which the medical conditions and symptoms of various diseases can be referred(47).during the Jan 2002 SNOMED CT was released, the International Health Terminology Standards Development Organisation (IHTSDO) maintains and promotes this to the clinical sector. SNOMED coding was mostly used for research purposes. 19 countries in the world uses this SONOMED CT for maintaining the clinical records(48)
HISTORY IN THE DEVELOPMENT OF THE SONMED (46)
| YEAR | VERSIONS OF SNOMED |
| 1965 | SNOP |
| 1974 | SNOMED |
| 1979 | SNOMED II |
| 1993 | SNOMED Version 3.0 |
| YEAR | VERSIONS OF SNOMED |
| 1997 | LOINC codes integrated into SNOMED |
| 1998 | SNOMED Version 3.5 |
| 2000 | SNOMED RT |
| 2002 | SNOMED CT |
CONCLUSION:
The usage of medical coding in the healthcare sector has made it easier for the collection of patient data regarding a disease diagnosis. So the coding system like ICD, CPT, and SNOMED. ICD –10 system of coding has reduced the coding time for the coder. ICD-10 and NTP have made the development of the ICD-11 model. CPT system has been an effective and efficient recording delivery of medical procedures performed by the physician. SNOMED CT model has provided great opportunities in understanding automated medical coding. Thus the usage of the different system of medical coding in the clinical sector and medical had paved a great improvement in the collection of data regarding healthcare sector by diagnosing various diseases and storage of information in research field.
REFERENCES:
- Eichelberg M, Aden T, Riesmeier J, Dogac A, Laleci GB. A survey and analysis of electronic healthcare record standards. Acm Computing Surveys (Csur). 2005 Dec 1;37(4):277-315.
- Escobar GJ, Turk BJ, Ragins A, Ha J, Hoberman B, LeVine SM, Ballesca MA, Liu V, Kipnis P. Piloting electronic medical record–based early detection of inpatient deterioration in community hospitals. Journal of hospital medicine. 2016 Nov;11:S18-24.
- Fraser HS, Biondich P, Moodley D, Choi S, Mamlin BW, Szolovits P. Implementing electronic medical record systems in developing countries. Informatics in primary care. 2005 Jun 1;13(2).
- Ferrao JC, Oliveira MD, Janela F, Martins HM. Clinical coding support based on structured data stored in electronic health records. In2012 ieee international conference on bioinformatics and biomedicine workshops 2012 Oct 4 (pp. 790-797). IEEE.
- Berner ES. Clinical decision support systems. New York: Springer Science+ Business Media, LLC; 2007.
- Yan Y, Fung G, Dy JG, Rosales R. Medical coding classification by leveraging inter-code relationships. InProceedings of the 16th ACM SIGKDD international conference on Knowledge discovery and data mining 2010 Jul 25 (pp. 193-202).
- Stanfill MH, Williams M, Fenton SH, Jenders RA, Hersh WR. A systematic literature review of automated clinical coding and classification systems. Journal of the American Medical Informatics Association. 2010 Nov 1;17(6):646-51.
- Heywood NA, Gill MD, Charlwood N, Brindle R, Kirwan CC, Allen N, Charleston P, Coe P, Cunningham J, Duff S, Forrest L. Improving accuracy of clinical coding in surgery: collaboration is key. Journal of Surgical Research. 2016 Aug 1;204(2):490-5.
- Dixon J, Sanderson C, Elliott P, Walls P, Jones J, Petticrew M. Assessment of the reproducibility of clinical coding in routinely collected hospital activitydata: a study in two hospitals. Journal of Public Health. 1998 Mar 1;20(1):63-9.
- Wu P, Gifford A, Meng X, Li X, Campbell H, Varley T, Zhao J, Carroll R, Bastarache L, Denny JC, Theodoratou E. Mapping ICD-10 and ICD-10-CM codes to phecodes: workflow development and initial evaluation. JMIR medical informatics. 2019 Nov 29;7(4):e14325.
- Cartwright DJ. ICD-9-CM to ICD-10-CM codes: what? why? how?.
- Wetterling T, Kanitz RD, Borgis KJ. Comparison of different diagnostic criteria for vascular dementia (ADDTC, DSM-IV, ICD-10, NINDS-AIREN). Stroke. 1996 Jan;27(1):30-6.
- Roberts RF, Innes KC, Walker SM. Introducing ICD-10-AM in Australian hospitals. The Medical Journal of Australia. 1998 Oct 1;169(S1):S32-5.
- Dong H, Falis M, Whiteley W, Alex B, Matterson J, Ji S, Chen J, Wu H. Automated clinical coding: what, why, and where we are?. NPJ digital medicine. 2022 Oct 22;5(1):1-8.
- Ramalho A, Souza J, Freitas A. The use of artificial intelligence for clinical coding automation: a bibliometric analysis. InInternational Symposium on Distributed Computing and Artificial Intelligence 2020 Jun 17 (pp. 274-283). Springer, Cham.
- Smith NA, Livina VN, Byford R, Ferreira F, Yonova I, de LUSIGNAN S. Automated Differentiation of Incident and Prevalent Cases in Primary Care Computerised Medical Records (CMR). InMIE 2018 Jan 1 (pp. 151-155).
- Dong H, Falis M, Whiteley W, Alex B, Matterson J, Ji S, Chen J, Wu H. Automated clinical coding.
- Catling F, Spithourakis GP, Riedel S. Towards automated clinical coding. International journal of medical informatics. 2018 Dec 1;120:50-61.
- Eichelberg M, Aden T, Riesmeier J, Dogac A, Laleci GB. A survey and analysis of electronic healthcare record standards. Acm Computing Surveys (Csur). 2005 Dec 1;37(4):277-315.
- Sorte BW, Joshi PP, Jagtap V. Use of artificial intelligence in software development life cycle—a state of the art review. International Journal of Advanced Engineering and Global Technology. 2015 Apr;3(3):398-403.
- Torres JM, Lawlor J, Colvin JD, Sills MR, Bettenhausen JL, Davidson A, Cutler GJ, Hall M, Gottlieb LM. Icd social codes. Medical care. 2017 Sep 1;55(9):810-6.
- Stausberg J, Lehmann N, Kaczmarek D, Stein M. Reliability of diagnoses coding with ICD-10. International journal of medical informatics. 2008 Jan 1;77(1):50-7.
- Wing TL. ICD-10 medical coding: The role of perioperative services in addressing implementation challenges. AORN journal. 2016 Feb 1;103(2):177-88.
- Chen PF, Wang SM, Liao WC, Kuo LC, Chen KC, Lin YC, Yang CY, Chiu CH, Chang SC, Lai F. Automatic ICD-10 coding and training system: deep neural network based on supervised learning. JMIR Medical Informatics. 2021 Aug 31;9(8):e23230.
- Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi JC, Saunders LD, Beck CA, Feasby TE, Ghali WA. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Medical care. 2005 Nov 1:1130-9.
- Henderson T, Shepheard J, Sundararajan V. Quality of diagnosis and procedure coding in ICD-10 administrative data. Medical care. 2006 Nov 1:1011-9.
- Sundararajan V, Quan H, Halfon P, Fushimi K, Luthi JC, Burnand B, Ghali WA, International Methodology Consortium for Coded Health Information (IMECCHI). Cross-national comparative performance of three versions of the ICD-10 Charlson index. Medical care. 2007 Dec 1:1210-5.
- Hohl CM, Karpov A, Reddekopp L, Stausberg J. ICD-10 codes used to identify adverse drug events in administrative data: a systematic review. Journal of the American Medical Informatics Association. 2014 May 1;21(3):547-57.
- Bowman SE. Why ICD-10 is worth the trouble. Journal of AHIMA. 2008 Mar;79(3):24-9.
- Colladay D, Kostelecký VA. CPT violation and the standard model. Physical Review D. 1997 Jun 1;55(11):6760.
- Kostelecký VA, Russell N. Data tables for Lorentz and C P T violation. Reviews of Modern Physics. 2011 Mar 10;83(1):11.
- Li F, Jiang T, Li Q, Ling X. Camptothecin (CPT) and its derivatives are known to target topoisomerase I (Top1) as their mechanism of action: did we miss something in CPT analogue molecular targets for treating human disease such as cancer?. American journal of cancer research. 2017;7(12):2350.
- Kostelecký VA, Potting R. CPT and strings. Nuclear Physics B. 1991 Aug 5;359(2-3):545-70.
- Banuls MC, Bernabeu J. Studying indirect violation of CP, T and CPT in a B-factory. Nuclear Physics B. 2000 Dec 4;590(1-2):19-36.
- Dotson P. CPT® codes: what are they, why are they necessary, and how are they developed?.
- Thorwarth Jr WT. CPT®: an open system that describes all that you do. Journal of the American College of Radiology. 2008 Apr 1;5(4):555-60.
- Hirsch JA, Leslie-Mazwi TM, Nicola GN, Barr RM, Bello JA, Donovan WD, Tu R, Alson MD, Manchikanti L. Current procedural terminology; a primer. Journal of neurointerventional surgery. 2015 Apr 1;7(4):309-12.
- White SC. New Audiology CPT Category III Codes. The ASHA Leader. 2010 Mar;15(3):5-.
- Rubenstein J, Painter M. Watch for these urology-related CPT codes this January.
- Kuo TY, Manaker S. Reimbursement strategies and CPT codes for device development. Academic entrepreneurship for medical and health sciences. 2019;1.
- https://www.americanmedicalcoding.com/
- Cornet R, de Keizer N. Forty years of SNOMED: a literature review. BMC medical informatics and decision making. 2008 Oct;8(1):1-6.
- Stearns MQ, Price C, Spackman KA, Wang AY. SNOMED clinical terms: overview of the development process and project status. In Proceedings of the AMIA Symposium 2001 (p. 662). American Medical Informatics Association.
- Lee D, Cornet R, Lau F, De Keizer N. A survey of SNOMED CT implementations. Journal of biomedical informatics. 2013 Feb 1;46(1):87-96.
- Chang E, Mostafa J. The use of SNOMED CT, 2013-2020: a literature review. Journal of the American Medical Informatics Association. 2021 Sep;28(9):2017-26.
- Wang AY, Sable JH, Spackman KA. The SNOMED clinical terms development process: refinement and analysis of content. InProceedings of the AMIA Symposium 2002 (p. 845). American Medical Informatics Association.
- Stearns MQ, Price C, Spackman KA, Wang AY. SNOMED clinical terms: overview of the development process and project status. InProceedings of the AMIA Symposium 2001 (p. 662). American Medical Informatics Association.
- Lee D, de Keizer N, Lau F, Cornet R. Literature review of SNOMED CT use. Journal of the American Medical Informatics Association. 2014 Feb 1;21(e1):e11-9.
Softwares used by our Employees.
(Ready to get training on other softwares)





